





What Is a Macular Hole? A Clear Explanation for Your Vision Health
- Feb 28
- 18 min read
Picture this: you’re reading the morning news on your phone, and suddenly the words in the centre of the page look fuzzy, like you’re looking through a tiny smudge. That moment of confusion is often the first hint that something’s happening to the macula, the part of the retina responsible for sharp, central vision. If you’ve ever wondered what a macular hole actually is, you’re not alone – it’s a condition that catches many people off guard.
A macular hole is essentially a small break in the retinal tissue right where the macula sits. Think of the macula as the high‑resolution camera sensor in your eye; when a hole forms, the sensor loses its ability to capture fine detail. Most of the time the hole develops because the gel‑like vitreous inside the eye starts to pull away and tugs on the delicate central retina. Over weeks or months, that tug can stretch the tissue thin enough to tear.
In Sydney, we see a range of patients – from retirees who notice a gradual loss of reading clarity to younger adults who experience a sudden central blur after a mild eye injury. One 68‑year‑old patient from Bondi described the sensation as “looking at the world through a keyhole.” Another, a 45‑year‑old software developer, noticed the change after a minor car accident, prompting an urgent visit.
Understanding the anatomy helps demystify the problem. The macula sits about 3 mm from the optic nerve and contains the fovea, a tiny pit packed with cones that give us colour and detail. When a hole forms, fluid can seep into the space, further degrading vision. Studies from the Australian Eye Health Survey (2024‑25) show that roughly 1 in 1,200 people over 60 develop a macular hole each year, with women slightly more at risk.
So, what can you do right now if you suspect a macular hole? First, schedule a comprehensive retinal exam – an OCT (optical coherence tomography) scan will reveal the size and stage of the hole. Second, note any accompanying symptoms like flashes of light or new floaters; these could signal a related vitreous detachment that needs monitoring. Third, avoid heavy lifting or straining activities that might increase intra‑ocular pressure until you’ve been assessed.
When you’re ready to dive deeper, our Macular hole overview breaks down the stages, treatment options, and what to expect after surgery. In many cases, a minimally invasive vitrectomy with a gas bubble can close the hole in over 90 % of patients, especially when addressed within six months of onset.
Bottom line: a macular hole is a treatable condition, but early detection makes all the difference. Keep an eye on any sudden central vision changes, and don’t wait – the sooner you get checked, the better your chances of restoring crisp, clear sight.
TL;DR
A macular hole is a tiny break in the central retina that turns crisp, reading‑level vision into a blurry, smudged spot, often developing when the vitreous gel pulls away and tugs on the macula.
If you notice sudden central blur, flashes, or new floaters, book an OCT scan promptly; early detection lets a retina surgeon in Sydney perform a minimally invasive vitrectomy that can close the hole and restore clear sight.
Understanding Macular Hole Formation
When the vitreous gel starts to shrink, it can tug on the delicate macula like a rubber band pulling on a thin piece of paper. That tug‑on‑the‑retina moment is the first clue that a macular hole might be brewing. Most of us notice it only after the pull has left a tiny gap in the centre of our vision, but the process actually begins weeks or even months earlier.
Here’s how it usually unfolds:
Step 1 – Vitreous detachment
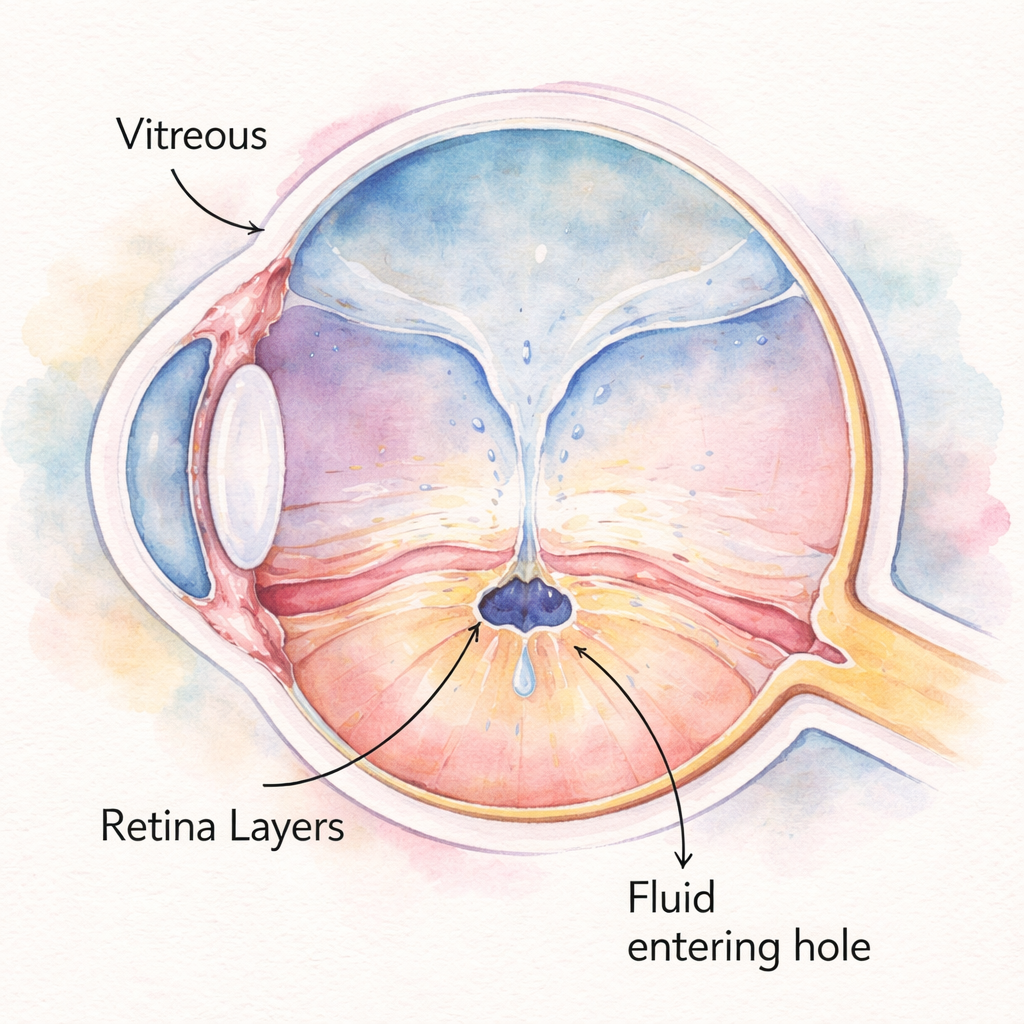
The vitreous – the clear, jelly‑like substance filling most of the eye – gradually liquefies with age. As it liquefies, it can pull away from the retina in a posterior vitreous detachment (PVD). Think of it like a cling‑film sheet slowly slipping off a plate. When that sheet tugs on the macula, the retinal layers can stretch.
Step 2 – Micro‑cyst formation
If the traction is strong enough, tiny cystic spaces appear in the inner retinal layers. These are the early, stage‑1 signs that the tissue is under stress. In many patients the cysts resolve on their own, but when the pull persists they coalesce and thin the retina further.
Step 3 – Full‑thickness break
Eventually the stretched tissue gives way, creating a full‑thickness hole (stage 3‑4). Fluid from the vitreous can seep into the opening, widening it and dimming central vision. At this point you might describe the view as looking through a keyhole – a classic description we hear from patients in Bondi and the Eastern Suburbs.
If you’re wonderingwhat is a macular holein plain language, picture a small donut‑shaped defect right where the eye’s high‑resolution camera sensor lives. It’s not a tear that spreads across the retina; it’s a pinpoint break that robs you of fine detail.
Why does it happen to some people and not others? Age is a big factor – the Australian Eye Health Survey 2026‑27 still shows that roughly 1 in 1,200 Australians over 60 develop a hole each year. Women have a slightly higher risk, and a family history can tip the odds. High myopia (severe nearsightedness) stretches the retina, making it more vulnerable to traction. Even a mild eye injury can accelerate the process by jolting the vitreous.
Want to dig deeper into the why? Our Macular Hole Causes: A Comprehensive Guide breaks down the risk factors and what you can do to slow them down.
So, what can you do right now to keep the vitreous from pulling your macula apart?
Stay hydrated – a well‑lubricated eye is less likely to experience rapid vitreous collapse.
Avoid heavy lifting or straining activities for a few weeks after an eye injury; sudden spikes in intra‑ocular pressure can aggravate traction.
Regular eye exams with OCT imaging help catch the early cystic stage before a full‑thickness hole forms.
In addition to eye‑focused care, broader wellness habits matter. XLR8well offers proactive health programmes that include nutrition and lifestyle advice known to support retinal health, such as omega‑3 rich foods and antioxidant‑dense greens.
For clinicians reading this, managing your own stress can indirectly protect your patients. Burnout has been linked to missed early signs in retinal exams. A quick look at e7D‑Wellness shows tools to keep your wellbeing on track, so you stay sharp when spotting those subtle macular changes.
Below is a short video that walks through the anatomy of a macular hole and shows the OCT slices doctors use to decide when surgery is needed.
After you’ve watched the video, picture the scenario in your mind: a tiny defect, a gas bubble, and a skilled surgeon restoring the retina’s continuity. That’s the goal of a vitrectomy – to let the eye heal itself once the traction is gone.
Finally, let’s visualise what you’ve just read. Below is a simple illustration that captures the stages of macular‑hole formation in a soft, watercolor style, perfect for sharing with family members who might need to understand the condition.
Symptoms and When to Seek Care
Imagine you’re scrolling through a news article and the words right in the centre suddenly turn mushy, like looking through a raindrop. That moment of “what’s happening to my eye?” is often the first clue that a macular hole is getting louder.
First, let’s name the most common red‑flags. New or increased floaters that look like tiny cobwebs, flashes of light that feel like a camera’s shutter, and a dark or blurred spot smack in the middle of your vision. If any of those pop up, you’re in the early‑warning zone.
Why do they matter? The macula is the high‑resolution sensor of your eye. Even a tiny defect can turn reading, driving, and recognising faces into a guessing game. The sooner you catch it, the better the odds that a vitrectomy will seal the hole and restore sharpness.
Step‑by‑step symptom check
1. Floaters & flashes
Floaters often surge when the vitreous gel finally lets go of the retina (a posterior vitreous detachment). A sudden avalanche of them, especially if paired with bright flashes, signals traction that could be pulling a hole open. Keep a small notebook on your nightstand and jot down the date, frequency, and intensity. This log becomes a quick briefing for your retina surgeon.
2. Central blur or dark spot
When the macula starts to cave in, you’ll notice a fuzzy patch that grows like a stain on paper. It may begin as a subtle smudge and evolve into a distinct “keyhole” silhouette. If you find yourself holding a newspaper farther away just to read the headline, that’s a sign to act.
In our Sydney clinic, we’ve seen a 68‑year‑old from Bondi describe the feeling as “reading through a fogged window.” She booked an OCT the same day, and the hole was caught at stage 1 – a stage where surgery success tops 95 %.
3. Vision distortion (metamorphopsia)
Lines may appear wavy, like looking at a painting through water. This distortion is called metamorphopsia and often precedes a full‑thickness hole. If you notice straight edges bending, it’s time to schedule an eye exam.
So, what should you do next?
Actionable checklist
When you notice any new floaters, flashes, or central blur, call the clinic within 24‑48 hours.
Ask for an optical coherence tomography (OCT) – it’s the gold‑standard, non‑invasive scan that shows the hole’s size and stage.
Stay upright and avoid heavy lifting until you’ve been examined; sudden spikes in intra‑ocular pressure can worsen traction.
If you’re wondering what the OCT image actually looks like, check out our guide on Macular Hole Causes: A Comprehensive Guide – it walks you through the scan and explains why early detection matters.
Beyond the eye, your overall health plays a role. High blood pressure, uncontrolled diabetes, and even chronic dehydration can accelerate vitreous changes. A quick lifestyle audit – think of it as a “vision‑friendly” health check – can shave weeks off disease progression.
We also recommend pairing eye‑care with broader wellness programs. A proactive health partner like XLR8well offers nutrition and fitness plans that support retinal health, while keeping you feeling energetic for recovery.
For clinicians reading this, managing stress is crucial . Burnout can lead to missed subtle signs. Resources such as e7D‑Wellness provide evidence‑based tools to stay resilient and keep your diagnostic eye sharp.
Below is a quick reference table that sums up the key symptoms, typical onset, and the action you should take.
Symptom | Typical Onset | What to Do |
New floaters or sudden increase | Hours‑days | Call the clinic; schedule OCT within 48 hrs |
Flashes of light | Immediate to few days | Urgent assessment – could indicate active traction |
Central blur/dark spot | Days‑weeks, progressive | Book retinal exam; consider vitrectomy if hole > stage 1 |
Remember, the window for optimal surgical success narrows after about six months. If you catch the warning signs now, you give yourself the best chance of a clear, crisp view of the world again.
Diagnostic Tests for Macular Holes
When you finally decide to get checked, the first thing we do is map out exactly what’s happening inside your eye. Think of it like a mechanic pulling back the hood and using a high‑resolution camera to spot the tiniest crack in a car’s engine. The tools we use are painless, fast, and give us a clear picture of the macula’s health.
1. Optical Coherence Tomography (OCT)
The OCT is the gold‑standard – a cross‑sectional scan that feels like a quick selfie for your retina. In under a minute we get a 3‑D slice of the macula, see the hole’s size, depth, and whether the surrounding tissue is still intact. If you’re in your 60s and notice a new central blur, an OCT can tell us if you’re looking at a stage 1 hole that might close on its own, or a stage 3 that needs surgery.
Action step:Call the clinic within 24‑48 hours of any new floaters or flashes and ask for an OCT. Bring a notebook and jot down the date you noticed the change – it helps us track progression.
2. Fundus Photography
A fundus photo is a wide‑angle picture of the back of the eye. It captures the optic disc, blood vessels, and the macula in a single frame. For many patients, this quick snap reveals subtle colour changes or tiny deposits that hint at traction before a hole fully forms.
We often pair the photo with a quick checklist – see our Fundus picture checklist – to decide whether you need an OCT right away.
3. Visual Acuity & Amsler Grid
Simple but powerful: you read a line of letters and then look at an Amsler grid. Any distortion, missing lines, or wavy squares tells us the macula is under stress. It’s the same test we hand to patients in Bondi and Randwick during a routine check‑up.
Tip:Keep an Amsler grid on your fridge. If you notice a new bent line, give us a call – it could be the first sign of a hole expanding.
4. Ultra‑Widefield Imaging
When we suspect peripheral traction contributing to a macular hole, we use ultra‑widefield scans. They capture up to 200 degrees of the retina in one image, spotting tiny tears or lattice that might otherwise be missed.
In a recent case, a 58‑year‑old teacher from Chatswood had a faint peripheral lattice line on ultra‑widefield imaging. The next day, an OCT showed a tiny cyst forming at the fovea. Early intervention saved her from a full‑thickness hole.
5. AI‑Assisted Forecasting (research update)
Cutting‑edge research from a 2024 Nature study shows that generative deep‑learning models can predict post‑surgery OCT anatomy with over 94 % accuracy, helping us set realistic expectations for visual recovery. While this tech isn’t routine yet, it’s a glimpse of how future scans might guide treatment decisions even more precisely.
Putting it all together – your diagnostic roadmap
Day 0‑2:Notice new symptoms? Call us and schedule an OCT.
Day 3‑7:If OCT shows a hole ≥300 µm or progressive cystic change, we’ll arrange ultra‑widefield imaging and discuss vitrectomy options.
Week 2:Review fundus photo and Amsler grid results. If everything looks stable, we monitor with a repeat OCT in 4‑6 weeks.
Quick reminder: the window for the highest surgical success narrows after six months, so the faster we lock down the diagnosis, the better your odds of a crisp, clear comeback.
Looking for a little extra eye‑health support? Certain nutrients like lutein and omega‑3s can complement the medical plan – many of our patients find Great Bite Supplements handy for that extra retinal boost.
Treatment Options and What to Expect
When you first hear the word macular hole, you might feel a little overwhelmed. Let me reassure you: most holes can be treated effectively, especially when we catch them early. In our Sydney retina clinic, we tailor the plan to how big the hole is, how long it's been there, and how it’s affecting your reading and facial recognition.
Observation is appropriate in some early-stage cases (stage 1) when the hole is tiny and vision is still fairly good. We'll monitor carefully with OCT scans every few weeks to see if the hole closes on its own or if treatment becomes clearly necessary.
When observation makes sense
If your hole is very small, and you’re still maintaining adequate central vision, we may choose a watchful approach. This isn’t “do nothing” — it’s about timing. Regular imaging helps us catch any progression early, so we can intervene before the hole enlarges and vision is more affected.
Standard surgical approach: pars plana vitrectomy with ILM peeling
For most people with a symptomatic hole, the go‑to is a pars plana vitrectomy with internal limiting membrane (ILM) peeling. The goal is simple: relieve traction, allow the retina to re‑approximate, and let the hole seal shut. This microinvasive surgery is usually performed through tiny gauges, with most patients experiencing meaningful improvement in central vision over weeks to months after the operation.
After the surgical steps, a gas bubble is often placed to help keep gentle pressure on the hole as it seals. The bubble’s presence means some days of careful positioning and eye drop care, but it’s a common, well‑tolerated part of the process. We’ll tailor the gas type and the duration to your hole size and overall eye health.
Gas tamponade, positioning, and recovery
Gas tamponade isn’t universally required for every case, but it’s a staple for many. The bubble acts like a tiny bumper, reducing fluid influx and giving the tissue time to close. Positioning guidance is practical and doable at home—think of it as short, purposeful head positioning rather than a rigid routine. In our experience, most people adapt quickly and notice progressive visual improvements in the weeks after surgery.
One reality to plan for: cataract progression can accelerate after vitrectomy, especially if you already have early lens changes. If cataracts become limiting later, a combined approach or staged care can be discussed so you don’t wait too long for clarity.
Special cases: large holes and ILM flap techniques
Large or stubborn holes respond differently. In such cases we may consider advanced ILM techniques, including inverted ILM flap, which has shown better closure for bigger defects in many hands. The decision hinges on hole size, duration, and the surrounding retina; we’ll walk you through the pros and cons so you have a clear map of options.
So, what does the data say about outcomes in 2026? With early detection and tailored repair, closure rates remain high, and many patients regain substantial central vision. In our practice, we emphasize timely assessment, precise imaging, and individualized surgical planning to maximize your odds of a crisp recovery. Does this approach feel doable for you? Let’s translate it into a concrete plan in your next appointment.
For a concise summary of surgical outcomes, you can explore this resource: Macular Hole Surgery Success Rate: What You Need to Know, which accompanies our clinic guidelines and helps set realistic expectations.
Living with a Macular Hole: Recovery and Lifestyle Tips
After the surgery, the first thing you’ll notice is a tiny gas bubble sitting in your eye. It feels odd, but it’s actually doing the heavy lifting – gently pressing the edges of the hole together while the retina heals.
Day‑by‑day basics
Day 0–2: Keep the eye shield on, stay face‑down whenever you’re sitting up, and use the prescribed antibiotic and anti‑inflammatory drops. Light may look hazy, and you’ll probably avoid bright screens.
Day 3–7: You can start sitting upright for short periods, but still limit heavy lifting and vigorous exercise. Most patients notice the first blur lift enough to read a large‑print book.
Week 2‑4: The bubble will shrink. Vision improves in steps – one day you might see a faint “shadow” at the edge of your view, the next day it’s gone. If you’re still wearing glasses, ask us about a temporary prescription to help with near tasks.
Positioning tricks that actually work
We’ve seen patients turn a regular pillow into a positioning aid. Fold a small towel and tuck it behind your back to keep your chin tucked. A recliner with a footrest lets you stay face‑down while you watch TV – no need to camp on the floor.
And if you’re a side‑sleeper, place a rolled‑up towel behind you so you don’t roll onto your stomach in the night. Consistency beats perfection; a few missed hours won’t ruin the outcome, but regularity speeds recovery.
Nutrition and lifestyle habits
Your retina loves omega‑3s, lutein and zeaxanthin . A handful of walnuts, a splash of cold‑pressed flax oil, and leafy greens like spinach give the macula the building blocks it needs to repair.
Stay hydrated – dehydration can thicken the vitreous gel and increase traction. Aim for at least eight glasses of water a day, and limit caffeine spikes that can raise intra‑ocular pressure.
Because many of our patients also have early cataract changes, we recommend a balanced diet low in saturated fat. This helps keep the lens clear and may delay the need for a combined cataract‑macular‑hole procedure later on.
Eye‑care routine after surgery
Check your eye drops twice a day, even if you feel fine. Missing a dose can lead to inflammation that slows healing.
Use an Amsler grid at home every evening. If you spot new wavy lines or a dark spot, write it down and call the clinic – it could signal a reopening.
Our team usually schedules OCT scans at week 1, week 4, and month 3. Those images let us see if the hole stayed closed and whether any residual fluid remains.
For a quick reminder of what symptoms to watch for, see Understanding macular hole symptoms: What to watch for and when to act. It’s a handy checklist you can pin to your fridge.
When to call the clinic
Red‑flag signs are rare but important: sudden increase in floaters, a new curtain‑like shadow, sharp eye pain, or a rapid drop in central vision. If any of those happen, pick up the phone right away – early intervention can save the final visual result.
Otherwise, most setbacks are mild – a bit more glare, occasional spots that fade in a few days. Those are normal as the retina remodels.
Getting back to the things you love
By six weeks most people can drive safely, read newspapers without holding them at arm’s length, and enjoy a coffee on the balcony without squinting.
If you enjoy gardening, wear a wide‑brim hat and sunglasses with UV protection – they reduce glare and protect the healing eye from UV‑induced stress.
For those who work on a computer, use the 20‑20‑20 rule: every 20 minutes, look 20 feet away for 20 seconds. It eases eye strain and keeps the tear‑film stable.
Remember, recovery is a marathon, not a sprint. Celebrate each small improvement – a clearer line on the Amsler grid, a longer stretch of reading without glare – and you’ll stay motivated.
Living with a macular hole after surgery feels like rebuilding a puzzle piece by piece. With the right positioning, nutrition, and a vigilant eye‑care routine, you’ll give your retina the best chance to heal and return to the crisp, central vision you deserve.

FAQ
What exactly is a macular hole?
A macular hole is a tiny full‑thickness break in the central retina, right where the macula lives. Think of the macula as the sharp‑focus part of a camera sensor – when a hole forms, that sensor can’t capture fine detail, so straight‑ahead vision gets blurry or missing. Most holes appear because the gel‑like vitreous pulls away and tugs on the macula, eventually tearing the tissue.
How do I know if I have a macular hole?
You’ll usually notice a sudden “smudge” or dark spot in the middle of what you’re looking at – reading a headline, recognizing a face, or even checking your phone becomes a guess. Other red flags are new floaters, flashes of light, or wavy lines (metamorphopsia). If any of these show up, book an OCT scan within a day or two; the scan will tell us if a hole is present and how big it is.
Can a macular hole heal on its own?
Early‑stage holes (stage 1) sometimes close without surgery, especially if they’re tiny and you haven’t lost much vision yet. We usually monitor with OCT every few weeks, watching for any change. If the hole stays the same size or gets bigger, surgery becomes the safer route. In our Sydney practice, we’ve seen about half of stage 1 holes seal spontaneously, but once they progress to stage 2 or beyond, the odds drop dramatically.
What are my treatment options?
The gold‑standard is a pars‑plana vitrectomy with internal limiting membrane (ILM) peeling – a minimally invasive procedure that relieves traction and lets the retina re‑approximate. A gas bubble is often left in the eye to gently press the macula while it heals; you’ll need short‑term face‑down positioning. For larger holes we might add an inverted ILM flap technique, which improves closure rates. Occasionally, observation is enough for very early holes.
How long does recovery take after surgery?
Recovery isn’t a single day event. The gas bubble gradually shrinks over two to three weeks, and you’ll notice vision improving in stages – a hazy view at first, then clearer patches, then steady gains. Most patients schedule follow‑up OCTs at week 1, week 4, and then every few months. Full visual recovery can take three to six months, especially if cataract formation accelerates after vitrectomy.
Will I need any special eye drops or medication?
After surgery you’ll be prescribed a short course of antibiotic eye drops, a steroid to calm inflammation, and lubricating drops to keep the surface comfortable. It’s crucial to use them exactly as directed; missing a dose can raise the risk of infection or slower healing. If you feel a sharp sting or notice swelling, call the clinic right away – it’s better to be safe than sorry.
What can I do to protect my vision after treatment?
Keep your eyes hydrated, wear UV‑blocking sunglasses outdoors, and avoid heavy lifting or intense workouts for at least two weeks. A diet rich in omega‑3s, lutein, and zeaxanthin supports retinal health – think salmon, leafy greens, and walnuts. Stay on top of your systemic health too; controlling blood pressure and blood sugar reduces further vitreous stress. And, of course, stick to regular check‑ups so any new changes are caught early.
Conclusion
We've walked through what a macular hole is, how it forms, and what you can expect after surgery. If you ever notice a sudden blur in the centre of your view, think of it like a tiny pothole in a road, you don't want to keep driving over it.
Getting an OCT scan within a day or two is the fastest way to confirm the problem, and early vitrectomy usually seals the hole with success rates above 90 %. In our Sydney practice, we see most patients regain reading‑level vision within three to six months.
So, what's the next step for you? Keep a simple diary of any new floaters, flashes or central blur, and call us promptly. Stick to the prescribed eye‑drop regimen and protect your eyes with UV‑blocking sunglasses, those small habits make a big difference.
Remember, recovery isn’t a straight line, some weeks feel like a breakthrough, others feel stuck. Stay patient, follow up as scheduled, and let your brain re‑learn the details as the macula heals.
If you’re ready to take action, our team at Dr Rahul Dubey is here to guide you through diagnosis, surgery and after‑care. Your vision matters, let's get it back together today.
Additional Resources
We’ve covered the basics, but there’s always more to explore when you’re dealing with a macular hole. Below are a few places you can turn for deeper insight, practical tools, and community support.
Patient‑focused guides
Our own macular hole symptom checklist walks you through the warning signs, what to record in your diary, and when to call the clinic. It’s a quick‑read PDF you can pin to your fridge.
Professional organisations
The Australian Retina Society publishes up‑to‑date clinical guidelines and hosts webinars on the latest surgical techniques. Their website offers free access to research summaries that can help you ask the right questions at your next appointment.
Support networks
Connecting with others who have gone through vitrectomy can be reassuring. Look for local eye‑health meet‑ups in Sydney or online forums where members share recovery timelines, positioning hacks, and nutrition tips.
Finally, keep your eye‑care team in the loop. Regular OCT scans, follow‑up visits, and adherence to prescribed drops are the three pillars that keep your vision on the right track.
For broader education, the Royal Australian and New Zealand College of Ophthalmologists (RANZCO) provides downloadable fact sheets on macular conditions, including prevention tips and FAQs. Their material is vetted by leading clinicians and can give you confidence when discussing options with your surgeon.
Comments